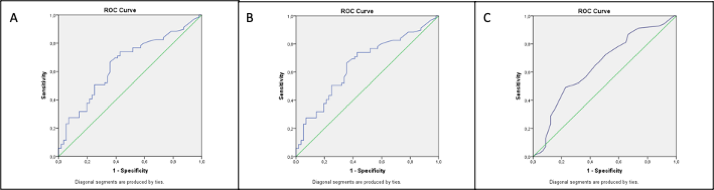
This study aimed to investigate epidemiological, clinical, and laboratory features of children with COVID-19 to identify predictors for pulmonary involvement. We conducted a retrospective, single-center study of pediatric COVID-19 at a tertiary care hospital in Turkey between December 2020 and June 2021. A total of 126 children (70 males, 55.6%) were examined during the study period. Their mean age was 74.73 ± 81.11 months (range, 1–216 months). The most frequent COVID-19 symptoms were fever (65.9%), cough (52.4%), and shortness of breath (18.3%). Ten patients required noninvasive mechanical ventilation. Sixty-nine patients (54.8%) had pneumonia. Longer duration of fever and the presence of cough were significantly associated with pulmonary involvement. In children with pneumonia, the C-reactive protein (CRP), procalcitonin levels, erythrocyte sedimentation rate (ESR), and viral load were significantly higher and lymphocyte and thrombocyte counts were significantly lower than in children without pneumonia. The cutoff viral load, CRP, and procalcitonin values for predicting pulmonary involvement were 26.5 cycle threshold (Ct; 95% confidence interval [CI], 0.54–0.74; sensitivity, 0.65; specificity, 0.56; area under curve [AUC]: 0.647, p = 0.005), 7.85 mg/L (95% CI, 0.56–0.75; sensitivity, 0.66; specificity, 0.64; AUC = 0.656; p = 0.003) and 0.105 ng/mL (95% CI, 0.52–0.72; sensitivity, 0.55; specificity, 0.58; AUC = 0.626; p = 0.02), respectively. High CRP, procalcitonin levels, ESR, and viral load and low lymphocyte and thrombocyte counts can predict pulmonary involvement in children with COVID-19, so better management may be provided for good prognosis.