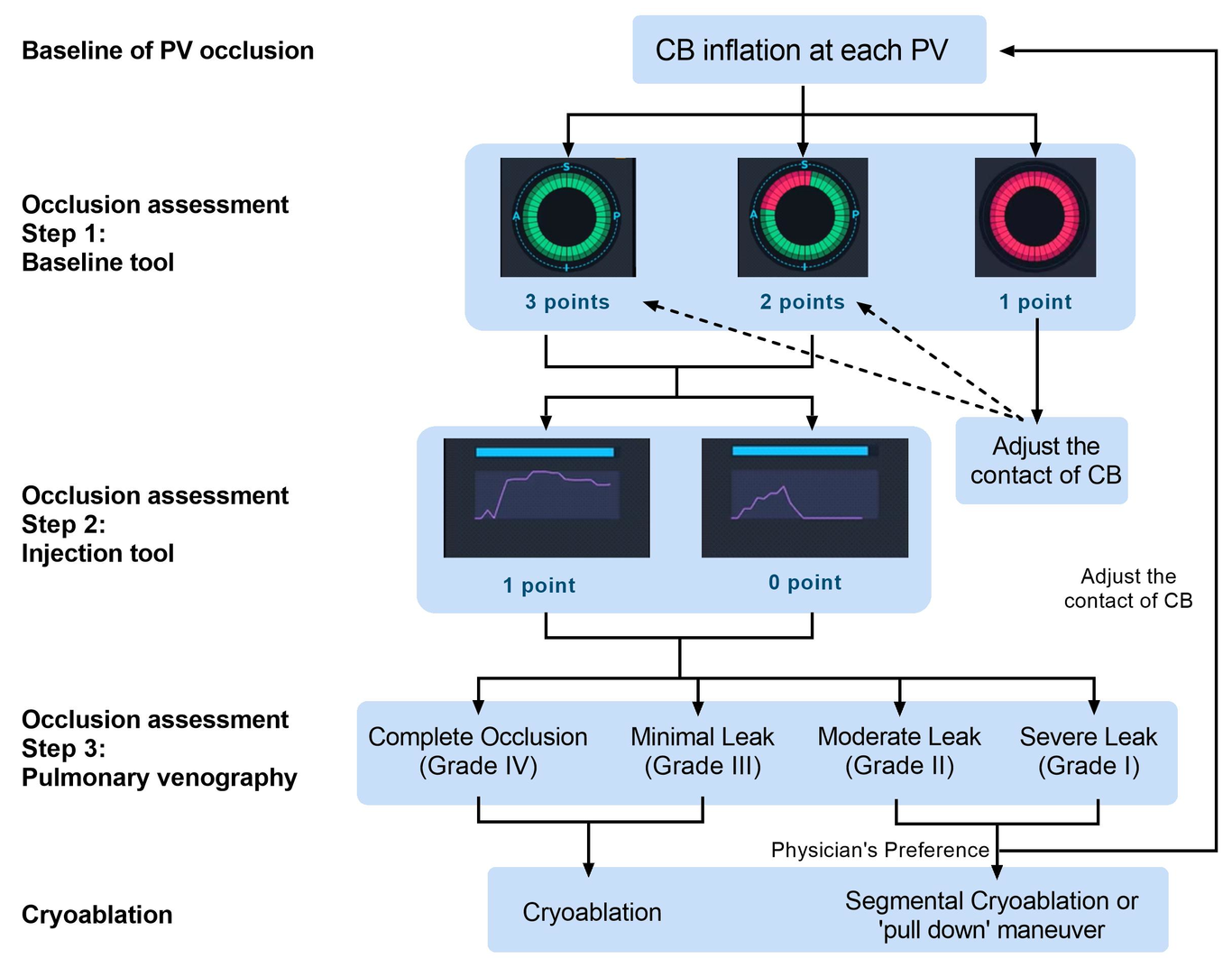
Background Optimal occlusion of pulmonary vein (PV) is essential for atrial fibrillation (AF) cryoballoon ablation (CBA). The aim of the study was to investigate the performance of two different tools for the assessment of PV occlusion with a novel navigation system in CBA procedure. Methods In consecutive patients with paroxysmal AF who underwent CBA procedure with the guidance of the novel 3-dimentional mapping system, the baseline tool, injection tool and pulmonary venography were all employed to assess the degree of PV occlusion, and the corresponding cryoablation parameters were recorded. Results In 23 patients (mean age 60.0 + 13.9 years, 56.5% male), a total of 149 attempts of occlusion and 122 cryoablations in 92 PVs were performed. Using pulmonary venography as the gold standard, the overall sensitivity, specificity of the baseline tool was 96.7% (95% CI 90.0% - 99.1%), and 40.5% (95% CI 26.0% - 56.7%), respectively, while the corresponding value of the injection tool was 69.6% (95% CI 59.7% - 78.1%), and 100.0% (95% CI 90.6% - 100.0%), respectively. Cryoablation with optimal occlusion showed lower nadir temperature (baseline tool: -44.3 + 8.4 ℃ vs -35.1 + 6.5 ℃, p < 0.001; injection tool: -46.7 + 6.4 ℃ vs -38.3 + 9.2 ℃, p < 0.001) and longer total thaw time (baseline tool: 53.3 + 17.0 s vs 38.2 + 14.9 s, p = 0.003; injection tool: 58.5 + 15.5 s vs 41.7 + 15.2 s, p < 0.001) compared with those without. Conclusions Both tools were able to accurately assess the degree of PV occlusion and predict the acute cryoablation effect, with the baseline tool being more sensitive and the injection tool more specific.