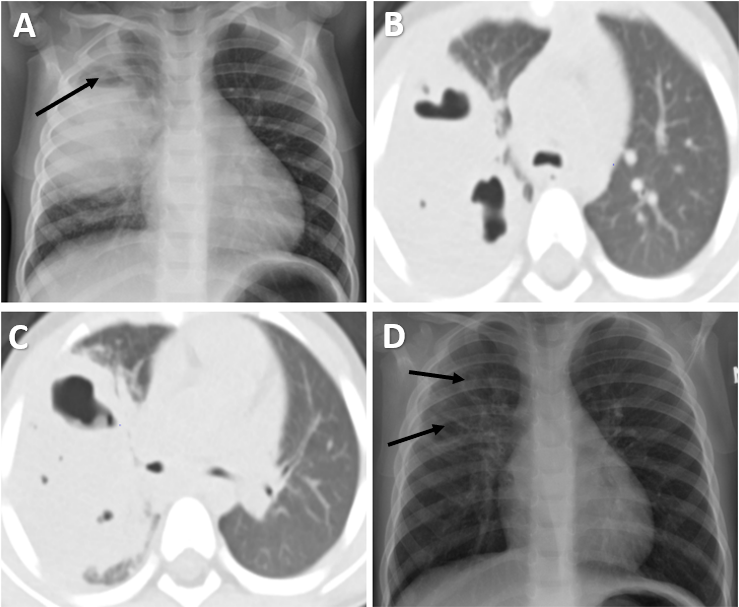
Late Development of Pneumatoceles in Necrotizing PneumoniaSila Y. Kocer 1, Nathan C. Hull MD2, D. Dean Potter, Jr. MD 3, Theresa Madigan MD 4, Jennifer M. Boland MD5 and Nadir Demirel MD 61Ondokuz Mayis University School of Medicine, Samsun, Turkey2Department of Radiology, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Surgery, Department of Surgery, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Infectious Diseases, Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Pulmonology, Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] : Sila Y. Kocer, Ondokuz Mayis University School of Medicine, Körfez, 55270 Samsun, Turkey. Email address: [email protected]. Tel.: +905514571963Conflict of interest: The authors declare no conflict of interest.Author contributions : Sila Y. Kocer: Writing – original draft. Nathan C. Hull: Writing – review and editing.D. Dean Potter Jr.: Writing – review and editing.Theresa Madigan: Writing – review and editing.Jennifer M. Boland: Writing – review and editing.Nadir Demirel: Writing – review and editing.Keywords : Lung cysts; complicated pneumonia; lobectomy; imaging; childrenTo the editor,Community-acquired pneumonia (CAP) is one of the most common serious infections in children, although it usually has a good prognosis1. Necrotizing pneumonia (NP), a rare but severe complication of CAP, consists of the destruction of the consolidated lung parenchyma, potentially leading to the formation of thin-walled cavities known as pneumatoceles 2. While they often resolve spontaneously without sequalae, progressively enlarging pneumatoceles have been reported 5. We report a pediatric case with an unusual course of pneumatocele development.A 3-year-old female with history of congenital hypothyroidism and mild asthma presented to her primary care physician for evaluation of intermittent fever for the past 6 days, with a maximum temperature of 38.8°C. She had a worsening wet cough and complained of chest pain while coughing. Lung examination was normal except for mild tachypnea. Based on the patient’s presentation, empiric oral amoxicillin 90 mg/kg/day was started for possible CAP. The patient presented to the clinic on day 6 of her antibiotic treatment with persistent low-grade fever and ongoing cough. She had normal vital signs, and there were no signs of respiratory distress. The lung examination revealed crackles at right lung fields. A chest X-ray (CXR) showed a large consolidation and an airspace with an air-fluid level in the right upper lobe (RUL) (Figure 1A). There was no pleural effusion. The patient was diagnosed with complicated pneumonia and was referred to our hospital.A chest computed tomography (CT) without intravenous (IV) contrast showed a large consolidation in the RUL with scattered internal cystic areas containing air-fluid levels (Figure 1B, C). These findings raised concern for NP, abscess, or congenital pulmonary airway malformation with superimposed pneumonia. Laboratory test results showed mild anemia (hemoglobin concentration of 10 g/dl), leukocytosis (white blood cell count of 14.1 x 109/L), thrombocytosis (platelet count of 752 x 109/L), and high C-reactive protein (CRP) (80 mg/L, normal: <5 mg/L). She was admitted and started on IV ceftriaxone and IV vancomycin. She remained afebrile during admission and was clinically well appearing. A nasal swab culture for Methicillin-resistant Staphylococcus aureus was negative, therefore, on day 2 of admission, IV vancomycin was discontinued. AStreptococcus pneumoniae urine antigen test was positive. Serologic testing for endemic fungi was negative. A QuantiFERON-TB Gold was indeterminate due to inadequate mitogen response. On day 3 of admission, in preparation for discharge, IV ceftriaxone was switched to oral cefdinir 14 mg/kg/day to complete a 4-week course. She remained afebrile and well after an additional 24-hour period of observation and was subsequently discharged.Towards the conclusion of her antibiotic course, a follow-up CXR showed near resolution of the RUL consolidative opacity with a few small residual lucencies in the RUL, presumed to be residual pneumatoceles (Figure 1D). She was asymptomatic without a cough, and her lung examination was normal. Inflammatory markers, including CRP and sedimentation rate, as well as white blood cell count and platelet count, were in the normal range. One month later, while the patient remained asymptomatic, a follow-up CXR revealed an enlarged pneumatocele (Figure 2A, B). A chest CT with IV contrast demonstrated a 7.2 x 5.3 x 7.6 cm air-filled cavity in the RUL (Figure 2C, D). No definite connection to the adjacent airways was seen on the chest CT. The patient then underwent a thoracoscopic right upper lobectomy. The procedure was challenging due to adhesions and bleeding (Figure 2E). The pathology examination of the resected lung tissue showed a simple fibrous-walled cyst devoid of epithelial lining, consistent with pneumatocele (Figure 2F). Gram stain, fungal smear, bacterial culture and fungal culture of the explanted lung tissue were negative. The patient made a full recovery, both radiologically and clinically.Patients with NP usually present with symptoms of CAP, unresponsiveness to initial outpatient treatment, such as high fever, cough, tachypnea, and general unwell appearance 1. The initial treatment of NP consists of IV antibiotics covering the most common etiologic agents of NP, which are known to be S. pneumoniae , Group AStreptococci and S. aureus . The optimal duration of antimicrobial therapy is not clearly defined; however, usually prolonged with a median duration of 4 weeks reported in the literature2, which aligns with guideline suggestions for therapy of empyema and parapneumonic effusion 3. Improvement in clinical and laboratory parameters usually allows for IV to oral antibiotic transition, which was accomplished relatively early for our patient, due to her less severe initial presentation and rapid clinical improvement. Pneumatoceles, air-filled cysts that can arise as a complication of NP, typically regress over weeks to months when NP is treated, but might require segmental or lobar resection if they become tense (exceeding more than 50% of the involved lobe), infected, or rupture 1. In our patient, many of the small pneumatoceles decreased in size after antibiotic treatment, with subsequent delayed and marked enlargement of one of them. A report on giant lung cysts emerging after NP suggested that, when patients remain clinically stable, treatment of pneumatoceles should be conservative with antibiotics alone regardless of the size of the cysts, as interventional procedures carry a risk of complications such as bronchopleural fistula 4. However, a study that proposed a treatment algorithm for pneumatoceles, recommended surgical resection for those that remained unresolved despite a conservative approach and gradually grew in size and wall thickness5. Our patient had no symptoms related to the pneumatocele. Nevertheless, it can be challenging to anticipate the progression of pneumatoceles, as they can enlarge enough to compromise respiration. The unusual expansion within a span of 1 month in our case, led to the decision of surgical resection.To summarize, we present a 3-year-old otherwise healthy girl with NP. After 4 weeks of antibiotic therapy, the right lung consolidations resolved and pneumatoceles decreased in size. However, one month later, while she remained clinically asymptomatic, a follow-up CXR revealed the progressive enlargement of a pneumatocele which eventually required surgical resection. Based on this experience, we suggest a close radiological follow-up of patients with post-infectious pneumatoceles, regardless of symptoms, until complete radiologic resolution is demonstrated.References1. de Benedictis FM, Kerem E, Chang AB, Colin AA, Zar HJ, Bush A. Complicated pneumonia in children. Lancet. 2020;396(10253):786–798. doi:https://doi.org/10.1016/s0140-6736(20)31550-62. Masters IB, Isles AF, Grimwood K. Necrotizing pneumonia: an emerging problem in children? Pneumonia (Nathan). 2017;9(1). doi:https://doi.org/10.1186/s41479-017-0035-03. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL, Mace SE, McCracken GH, Moore MR, et al. The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53(7):e25–e76. doi:https://doi.org/10.1093/cid/cir5314. Gross I, Gordon O, Cohen‐Cymberknoh M, Reiter J, Tsabari R, Gileles‐Hillel A, Erlichman I, Hevroni A, Shoseyov D, Kerem E. Giant lung cysts following necrotizing pneumonia: Resolution with conservative treatment. Pediatr Pulmonol. 2019;54(6):901–906. doi:https://doi.org/10.1002/ppul.243215. Imamoğlu M, Cay A, Koşucu P, Ozdemir O, Cobanoğlu U, Orhan F, Akyol A, Sarihan H. Pneumatoceles in postpneumonic empyema: an algorithmic approach. J Pediatr Surg. 2005;40(7):1111–1117. doi:https://doi.org/10.1016/j.jpedsurg.2005.03.048Authors and affiliations : Sila Y. Kocer 1, Nathan C. Hull MD 2, D. Dean Potter, Jr. MD3, Theresa Madigan MD 4, Jennifer M. Boland MD 5 and Nadir Demirel MD 61Ondokuz Mayis University School of Medicine, Samsun, Turkey2Department of Radiology, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Surgery, Department of Surgery, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Infectious Diseases, Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of Pediatric Pulmonology, Department of Pediatric and Adolescent Medicine, Mayo Clinic, Rochester, Minnesota, USA. Email address: [email protected] of interest: The authors declare no conflict of interest.