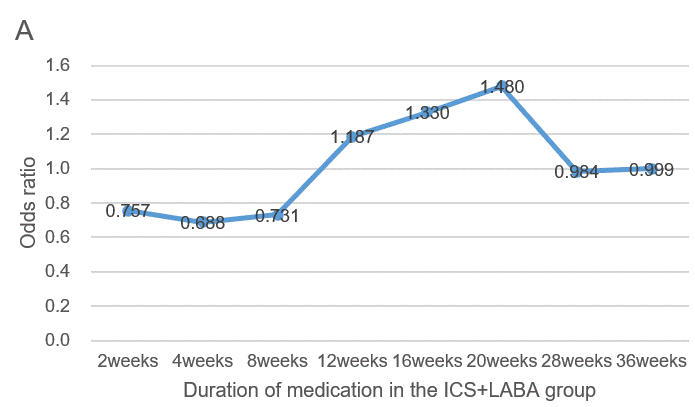
Treatment strategy of cough variant asthma in children–A retrospective longitudinal cohort study in ChinaTo the Editor,Cough variant asthma (CVA) is the most common cause of chronic cough, accounting for 41.95% of the causes of chronic cough among Chinese children, which greatly affects their learning, sleep, and quality of life[1,2]. About 40%–50% of CVA patients may eventually develop wheezing symptoms and progress to typical asthma if no appropriate and timely treatment is given [3]. However, the treatment plan and duration of children with CVA remain unclear. To this end, we performed retrospective longitudinal cohort study to explore the best therapeutic regimen and treatment duration of CVA in children.The study was approved by the Ethics Committee of Children’s Hospital Affiliated to Shandong University (The ethics protocol number is SDFE–IRB/T–2022075), which absolved the need for written informed consent. A total of 314 children with CVA were assigned to receive inhaled corticosteroid (ICS) combined with long-acting β2-agonist (LABA) group (group 1, n = 63), ICS combined with leukotriene receptor antagonist (LTRA) group (group 2, n = 186), ICS monotherapy group (group 3, n = 30), and LTRA monotherapy group (group 4, n = 35). Based on the causal diagram (Figure S1) model assumption, the marginal structure model and the Cox proportional hazard regression model were fitted to estimate the direct causal effect of the first medication on the efficacy and safety outcomes based on inverse probability weighting. Additional details on the methods are presented in the online supplementary.General Information of Children with CVA is shown in Table S1. Distribution of the number of patients changed from 0 weeks to 60 weeks with four treatment regimens is plotted in Figure S2. Results of superiority analysis with group 1 as the control (Table 1): ICS + LABA had the best effect within 8 weeks, followed by ICS + LTRA, whereas ICS alone and LTRA alone had the worst efficacy. With the extension of medication time, the efficacy of the ICS + LABA group was gradually lower than other groups in the same period. ICS alone was predominant at 8 weeks and beyond, followed by LTRA alone, whereas ICS + LABA and ICS + LTRA had the worst efficacy. Due to most of the guidelines recommend that the CVA treatment is for at least 8 weeks, we divided it into two parts with 8 weeks as the boundary[4-6]. There was no significant difference in therapeutic effects of the four treatment regimens within 8 weeks of diagnosis of CVA (Table S2). And the efficacy of ICS or LTRA alone was better than that of combination therapy after 8 weeks of diagnosis (Table S3).Table 1. Comparison of four medication regimens for CVA children at different courses.